National Maternity Voices invited anyone connected with a Maternity and Neonatal Voices Partnership to nominate a project undertaken in the last 2 years for one of our awards.
Below are the stars and other nominations for the ‘Co-production’ award: when staff and service users have worked together over an extended period to identify an issue and bring about improvements in the service. Presentations from the winners and contact emails for the MNVPs can be found on our main awards page.
Co-production Stars:
Induction Co production, Surrey and Sussex Healthcare MNVP: ongoing co-production which resulted in many changes
Multilingual Pre-term Birth Leaflet, Greater Manchester MNVP : Practical action based on deep understanding of marginalised service users
Personalised Care for NICU parents, Chelsea & Westminster MNVP: joining up maternity and neonatal care
Trisomy 21 Pregnancy & Beyond, Wirral MNVP: multidisciplinary work addressing the needs of a disadvantaged minority
Other Nominations:
Induction of Labour Video, Baywide MNVP
Maternity & Neonatal Infographic, Central Cheshire MNVP
Pregnancy Circles, Kernow MNVP
Breastfeeding Padlet, Staffordshire & Stoke on Trent MNVP
Neuroinclusive Maternity Passports, Coventry & Warwickshire MNVP
Induction of Labour project, Greater Manchester MNVP
Improvement to Discharge Process, Lister MNVP
Details of each project follow in order:
Co-production Stars:
Project: Induction Co production project
MNVP: Surrey and Sussex Healthcare MNVP
Star for: ongoing co-production which resulted in many changes
What? In the summer of 2024 a need was identified to review and address the volume of inductions at SASH. Based on anecdotal evidence, feedback from SASH and feedback from MNVP surveys we launched a co-production into Induction. In September 2024 we gathered together and discussed experiences of induction and what changes service users would like. 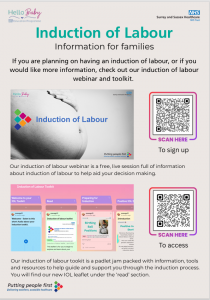
Following this the local induction process was revised and new information developed including a padlet. There was training for midwives, support workers and obstetric consultants and teams. Rotas were revised to ensure support for IOL bookings. The changes were piloted in April and come into full use in June 2026
Service user involvement: Women and birthing people gave feedback via a survey and 1:1 with MNVP Co-leads. Some attended on the co production day and shared their experiences in front of over 25 staff from SASH Maternity, Neonatal and external teams such as Health Visitors. During the day we split into groups to look at different elements of the pathway: information leaflets, local guidance, the national guidance and also any current support that there is or medical information for those experiencing or choosing induction of labour. After reviewing this, we created a range of actions as part of an 18 month co-production to drive change. Service users continued to be a part of our review and all of the work over 18 months. We also asked them how they would like to access information.
Staff involved: Former HOM Louise Frost, Current HOM Isata Tarawalla, current DOM Rosemary Idiagio, Consultant Midwife Emily Caulderon, Matron Amy Oehlers and a team of Matrons and Midwife
Benefits: The induction rate was circa 35% in September 2024 and has been 25-28% in the last 6 months. There is evidence to suggest inductions are occurring later than previously. Audit and review is ongoing. Revised processes include:
- New digital IOL booking form prompts evidence based discussion and informed decision making
- Outside guidance IOL reviewed daily by senior midwife + obstetrician before booking
- Prolonged pregnancy IOL offered between 41+0 – 41+5 (was from 40+5)
- Patient information updates New patient information leaflet includes postdates, outpatient IOL and large babies (LGA). New antenatal webinar for families (Happy Baby). Padlet resource created for women. New information on biomechanics, pain relief and relaxation. Translated material.
- Service pressures: Review of rotas, priority ratings added if IOL needs to be moved due to high activity, discussion of IOL at huddles.
Project: Multilingual Signs of Pre-term Birth Leaflet
Greater Manchester MNVPs
Star for: Practical action based on deep understanding of marginalised service users
What? Existing information regarding the signs and symptoms of pre-term birth was lengthy with an elevated reading age. Maternity services were particularly concerned that women from seldom heard communities were not always presenting to triage when experiencing signs of pre term birth. We spearheaded a collaborative project to create a resource specifically tailored for the diverse Greater Manchester (GM) community, but there was no set ‘agenda’ at the start of the project about what the resource might be.
The project centred on the development of a bespoke “Z-fold” leaflet—a discreet, portable card designed to be kept in a handbag. Unlike standard leaflets, this resource was built from the ground up by service users to ensure the language and visuals resonated with those from seldom-heard communities. Over 20,000 copies have been printed across Greater Manchester (with expressions of interest from other NHS trusts). This has been a long-term project. After 18-months, it is now available in seven languages, including Urdu, Arabic, Farsi, and Bengali, ensuring that vital safety information reaches those most at risk of health inequalities. Posters replicating the information are also now in use across GM Trusts (see top of one below) .

Service user involvement: We partnered with the Chai Project, conducting deep-dive engagement sessions with women’s groups in Trafford and Oldham. The Chai project specialises in working with asylum seeker, refugee and South Asian women. Service users highlighted significant barriers, noting that clinical terms like “pre-term” were often unrecognized; as one mother noted, “We might say baby comes early, but not pre-term.”
A major concern raised was the “smile and nod” phenomenon, where women felt pressured to appear as though they understood clinical information during appointments despite feeling overwhelmed. Families admitted they would avoid official websites, preferring to trust relatives, which risked delays in seeking urgent care. In response, women led the design process, deciding that a paper-based leaflet was the most appropriate resource for their community. The leaflet is a specific ‘Z’ fold design which those involved in the project told us was most appropriate for them, as it meant they felt comfortable taking the leaflet home as the key information was ‘hidden’ inside the folds.
We worked with a professional designed to create a range of visuals. The woman in our focus group selected the specific visuals and gave examples of simplified language and key messages they felt would be most effective. As one participant noted: “The images are understandable for anyone… and a reminder that you need to ring if you have any problems.”
Staff involved: GM MNVP acted as a bridge between the community and clinical leadership. We presented the feedback—specifically the disconnect between clinical terminology and community understanding—to NHS clinical leads (including Eileen Stringer, lead clinical midwife), Trust leadership, and system-level governance groups. We worked closely with Consultant Obstetricians to ensure that while the language was simplified, the clinical “red flags” remained accurate.
Staff were involved in reviewing the co-produced visuals, ensuring they aligned with hospital triage protocols. This also allowed us to explain the “smile and nod” barrier, helping staff realize why certain demographics were not presenting to triage when experiencing symptoms. Following the pilot, we escalated the project, resulting in the NHS adopting the leaflet as a formal resource across Greater Manchester. Clinical staff have embraced the change, with one Consultant Obstetrician noting: “This looks like a fantastic piece of work—I really like the format with the illustrations.”

Benefits: This practical service user-led project addressed real health inequalities. By replacing inaccessible, lengthy documents with the user-led and highly visual leaflet, we have directly improved the safety of mothers and babies. See youtube video here
The key benefits included:
- The right information, where it was most needed: By taking a co production approach and focussing on what women said they needed, we were able to identify the barriers that sometimes caused them to delay seeking medical advice at the first sign of pre-term birth. We used their ongoing feedback to create an information resource which was discreet, accessible and with clear, culturally-sensitive visuals.
- Improved Access: 20,000 copies printed in seven languages ensure that non-English speakers have the same access to emergency information as others.
- Safety & Equity: The clear “call to action” encourages women from seldom-heard communities to contact triage early, reducing the risk of unmanaged pre-term labour.
- System Efficiency: The leaflet has been been adapted and adopted by the South West region, who have further translated it into another six languages.
- Empowerment: It has shifted the local maternity culture toward true co-production, proving that clinical outcomes improve when service users are given the power to design the information which works for them.
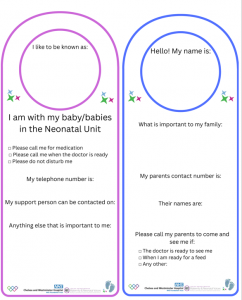
Project: Personalised Care and Support Plan for NICU/SCBU parents
Chelsea & Westminster MNVP
Star for: joining up maternity and neonatal care
What? Women and birthing people on Postnatal wards with their baby on NICU/SCBU, need care that is responsive to their needs. Care needs to be trauma informed, understanding of the experiences of families that don’t have their baby with them and recognition that they are the family of a baby who is a patient.

Our co-produced Postnatal Personalised Care and Support Plan (PCSP) aims to ensure that postnatal care and information is provided from the first opportunity. The plan offers information from the practical, such as phone numbers of Neonatal wards and medication and mealtimes on the Postnatal ward, to speaking openly about the emotions and feelings that families may have when their baby receives Neonatal Care. We are also proud of our ‘At a Glance’ page which details some practical and emotional aspects of care that are important to Neonatal families, using an ‘I/we’ perspective, which also serves as a quick resource for staff. There is also an Appendix of two signs that can be used both on the Postnatal ward and on the incubator/cot, when families are in either the Maternity or Neonatal area, updating each team on how to contact them and what’s important to the family. Families don’t separate their experiences into ‘Maternity’ and ‘Neonatal’; they want a cohesive care experience.
The information is provided in printed copy which enables families to read and digest at their own pace, and translate using resources such as Google Lens, if they prefer. This is responding to the ‘overwhelm’ that many families told us they felt, receiving so many updates or redirects to information.
The process was about eighteen months in the making, before we went ‘live’ a few months ago. (See Instagram Post @Chelwestmid_mnvp ) This is work in progress – we are continually working on consistency of accessibility, ensuring every family is better supported and understood.
 Service user involvement: We listened to a wide range of our service users in a range of formats over several months prior to beginning this project. There were Listening groups locally and regionally, we were on both our postnatal wards when families were still receiving care listening to ‘in the moment’ feedback, and we heard from service users who contacted us as an MNVP via either email or Teams calls. We continue to listen to service users and themes of feedback in relation to postnatal care for neonatal families, as well as completing ‘Temperature Checks’ on Postnatal Wards, to observe support in action and listen to the experiences of families.
Service user involvement: We listened to a wide range of our service users in a range of formats over several months prior to beginning this project. There were Listening groups locally and regionally, we were on both our postnatal wards when families were still receiving care listening to ‘in the moment’ feedback, and we heard from service users who contacted us as an MNVP via either email or Teams calls. We continue to listen to service users and themes of feedback in relation to postnatal care for neonatal families, as well as completing ‘Temperature Checks’ on Postnatal Wards, to observe support in action and listen to the experiences of families.
One mother who was on Postnatal ward during the development of the resource, said ‘Midwives are saying my baby is on Special Care. I wish they realised he’s ventilated and in Intensive Care.’ Her words reflect why service user voice and authentic co-production is so important when seeking to improve care experiences of families. The language used leaves lasting imprints on families, so when voices are centred, improvements can be sure to better reflect the needs of families, rather than assume
Staff involved: Multi disciplinary involvement that we are very proud of. This workstream has sat in our Cross-Site Postnatal Care Committee meeting, which was meeting monthly to discuss and hear progress, as well as continue the development and get this out on the wards. Representation has included, but is not limited to, Cross-Site Postnatal Ward Matrons, Cross -Site Lead Neonatal Nurse, Cross-Site Neonatal Matron and Infant Feeding Leads. We also sought support and input from our Consultant Clinical Psychologist.
Benefits: ‘This would have made such a difference to my care.’ A quote from one of our incredible service users who shared her very personal experience when her baby was admitted to NICU unexpectedly, and who we subsequently shared the PCSP with when it was nearing completion.
Too many families told us they miss postnatal mealtimes or pain relief, when with their baby on NICU/SCBU. Too many said they found it distressing in shared bays around others who have their baby with them, and wanted staff to know that if a private room is unavailable, the absence of being told the practical reason why they were on a shared ward, added to further upset and distress. Too many families told us they didn’t realise the emotions and feelings they were experiencing on Postnatal ward, when separated from their baby, were common amongst Neonatal families and wanted the conversation opened, as well as practical ways to support their baby on the Neonatal Unit from the first moment.
Our resource seeks to improve equity to postnatal care, as well as empower families with the information and resource they need to become partners in their baby’s care from Day 0. It seeks to improve consistency of access to information that doesn’t vary between staff teams.
The resource also benefits staff teams, who are able to understand the aspects of care that are important to families and practical ways to support them. Our resource importantly joins Maternity with Neonatal, responding to feedback that when services operate in silos, the families who receive care notice. The project has been shared with other London trusts and South West ODN; it has received a wide range of support and positive feedback. (The team are happy to share their PCP resource so long as they are credited)
Project: Trisomy 21 Pregnancy & Beyond
Wirral MNVP
Star for: multidisciplinary work addressing the needs of a disadvantaged minority
What? The project focused on improving the experiences of families navigating maternity and neonatal services following a diagnosis of Trisomy 21 (Downs). Feedback from local families highlighted inconsistencies in communication, limited emotional support, and a lack of a clear pathway for families and professionals following diagnosis, both antenatally and postnatally. Families described feeling overwhelmed, isolated, and unsure where to access information and support during an emotionally significant time.
Wirral MNVP led a co-production approach centred around lived experience. We engaged with 17 local families to better understand their experiences and identify themes, challenges, and opportunities for improvement. We brought together a wide range of stakeholders including local charities to support collaborative working and shared learning. A multi-agency task and finish group focused on developing a clearer and more compassionate pathway for families receiving a diagnosis of Trisomy 21. The project also contributed to the development of staff training as their experiences have been captured on film. (See Facebook Post). Reflective learning focused on compassionate communication, emotional support, and improving the experiences of families during complex and sensitive conversations.
Service user involvement: The issue was identified through direct feedback from families with lived experience of receiving and navigating a diagnosis of Trisomy 21 locally. Families shared experiences of inconsistent communication, a lack of emotional support, and uncertainty around available pathways and services following diagnosis. These conversations highlighted the need for more compassionate, joined-up, and family-centred approaches across the system. Service users were central to the project from the outset. The MNVP collaborated with local charity Sundowns, a small grass root organisation to help engage with 17 local families to gather detailed lived experience feedback and identify common themes, challenges, and opportunities for improvement. Families contributed through conversations, feedback discussions, and ongoing engagement throughout the project, helping shape priorities and recommendations. The feedback informed the development of a local task and finish group, pathway discussions, and staff training initiatives focused on compassionate communication and supporting families receiving complex diagnoses. The families experiences have also been captured on film and will be implemented across staff training, both online and in-person.
Staff involved: The project brought together a multi-agency group including obstetricians, paediatricians, neonatal nurses, midwives, perinatal mental health teams, health visitors, EDI leads, and local charities to support collaborative working and pathway development. Community and third-sector involvement helped ensure families’ experiences were considered holistically and that support extended beyond clinical care alone.
Benefits: The project improved collaboration across maternity, neonatal, paediatric, mental health, and community services to create a more joined-up and compassionate experience for families navigating a diagnosis of Trisomy 21. By centring lived experience, the work helped amplify the voices of families who can experience stigma, inconsistent communication, and variation in support. Feedback informed pathway discussions and staff training focused on compassionate communication and emotional support during complex diagnoses. Families highlighted the importance of “clearer information,” “more compassion,” and “joined-up support,” while professionals recognised the value of hearing lived experience directly to improve consistency and family-centred care across services.
Other Nominations:
Project: Induction of Labour Information Video
Baywide MNVP (Baywide MNVP Facebook Page )
What? The MNVP Lead heard that induction of labour was not a good experience for local families for several reasons. Service users co-produced an Induction of Labour (IOL) leaflet in 2024 with UHMBT, but there was very little impact. Families across Morecambe Bay continued to report variable experiences of induction.
Service user involvement: In 2025 the team developed an Induction of Labour survey to gather more tangible data via social media and direct to community groups and service users. Service users were also asked if they would like to get involved in an IOL stakeholder group. The stakeholder group has been working in partnership with the Consultant Midwife and In-house patient midwife Lead to develop an IOL script based on their shared experiences. These meetings have been wonderful to observe because it has provided an opportunity for all stakeholders to share their IOL experiences, and the senior midwife leads to listen to their voices, and together they have identified the best solutions that will be included in the video. The filming will be starting in June, and all the stakeholders will be using their voices to inform new mums to be about the Induction of Labour.
Staff involved: Lancashire and South Cumbria LMNS/ICB UHMBT – DoM/HoMs/QAS Midwife/Consultant Midwife/In-Patent Midwife.
Benefits: The IOL stakeholder engagement has empowered so many mums, their experiences have been shared, heard, and actions have been taken to improve IOL care across Morecambe Bay. The video will provide IOL guidance/factual information and personal experiences to support new mums to be and their families.
Project: Maternity & Neonatal Infographic
Central Cheshire MNVP
What? Families told us that local birth data felt inaccessible, difficult to interpret and sometimes anxiety provoking when presented without context. Some parents wanted transparent outcome data to support decision making. Others wanted a keepsake, humanised and something they could keep as a record.
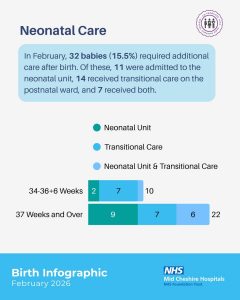
We also recognised that maternity data presentation is often maternity-centric, with neonatal outcomes and bereaved families less visibly represented. We wanted to ensure that neonatal care, transitional care and baby loss were given weight and respectful visibility within the resource.
Before designing the infographic itself, we undertook prolonged surveying and engagement conversations to understand how families actually use infographics. We explored whether they were viewed as keepsakes, decision-making tools, comparison resources, or reassurance tools. Only once we understood this did we refine the level of detail, structure, and tone of each section.
See all the infographic pages on the MNVP Facebook here or Instagram here
Service user involvement: Before designing the infographic, we undertook extended surveying and engagement to understand how families use this information. We explored whether infographics functioned primarily as keepsakes, comparison tools, reassurance aids, or decision-making resources. This allowed us to refine the level of detail and tone before focusing on individual sections. We then held iterative discussions with service users, shared draft versions for structured feedback to community groups and local families. Revised language to improve clarity and accessibility, ensured neonatal outcomes and transitional care were visibly represented, and that the ODN Parent Engagement Lead and PAG had oversight of our approach. Co-produced a baby loss acknowledgement statement with local bereaved families and SANDS. Worked closely with Trust maternity and neonatal leadership to verify data accuracy.
Multiple revisions were made following parent feedback, particularly around simplifying terminology and clearly explaining concepts such as VBAC and RCOG caesarean classification. The infographic was also launched alongside a further survey for feedback, to allow for adjustments and improvements moving forward.
Staff involved: From Mid Cheshire Hospitals NHS Foundation Trust (MCHFT): Catherine Warner, Divisional Quality Lead, Lydia Hassall, Digital Support Midwife, The Extended Maternity Team, Bereavement Midwife, Governance and data leads (role based input)
From the wider system: Victoria Walsh, Parent Engagement Lead, Operational Delivery Network (ODN), Joy Casewell, MNVP Lead, Melanie English, MNVP Deputy Lead, Stephanie Wood, MNVP Engagement Lead.
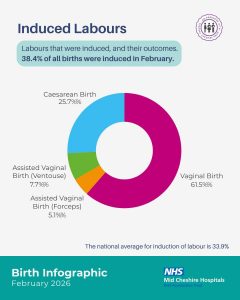 Benefits: The infographic balances transparency with reassurance, making clear that statistics describe proportions, not individual experiences. It has increased transparency of local maternity and neonatal outcomes, improved accessibility of complex audit data, supported informed antenatal decision-making, ensured neonatal care is visibly represented, acknowledged bereaved families, provided national context to support interpretation.
Benefits: The infographic balances transparency with reassurance, making clear that statistics describe proportions, not individual experiences. It has increased transparency of local maternity and neonatal outcomes, improved accessibility of complex audit data, supported informed antenatal decision-making, ensured neonatal care is visibly represented, acknowledged bereaved families, provided national context to support interpretation.
Ethnicity and demographic data will be added in future editions once we have refined and validated the data to ensure it is presented accurately and meaningfully.
Initial Feedback :
“ You’ve answered almost every question I normally tell people to ask about birth statistics. It’s refreshing to see this level of detail.”
“Using ‘unplanned’ rather than ‘emergency’ is such an important distinction. This helps people understand urgency versus perception.”
“The VBAC breakdown is incredible. I was genuinely surprised – in a good way.”
“The stats are far less enraging when they’re presented clearly and honestly.”
“I think it’s amazing there will be a whole page each month to acknowledge those little ones and their families”
“This will be such a valuable resource to help parents make informed decisions.”
Project: Pregnancy circles
Kernow MNVP
What? Pregnancy Circles is a model of group antenatal care genuinely designed with women. The project is rooted in lived experience, equity and community voice, ensuring that women and families shaped every stage of design, testing and refinement, especially those whose voices are least often heard. The MNVP lead brought together midwives, community groups, public health and families to co‑create a model that improves access, builds confidence and strengthens relationships. The Circles are improving engagement, continuity and belonging for women who often feel marginalised by traditional care. (We believe this project was undertaken more than 2 years ago and therefore does not meet the criteria for an award but include it here for readers interest)
Service user involvement: Identified as part of the REACH controlled trial of pregnancy circles. Evidence based – Improving early access to antenatal care, enhancing service user’s experience and reducing inequalities in outcomes. Brought together women from diverse backgrounds — including those who traditionally have the least influence over maternity services. Continuous feedback and shared decision‑making. Service users are involved not just at the start, but throughout.
Staff involved: Maternity Matron – Sam Gale Community Team Leader – Lizzie Anstey
Benefits: Co-design from the outset. Women from similar backgrounds were brought together, helping them build networks, share knowledge and feel more in control of their pregnancy journey — a key factor in reducing inequalities. By embedding face‑to‑face translators within every Circle, women with limited English proficiency could participate fully, ask questions, share experiences and shape the service. This moved them from the margins to the centre of the conversation. By offering group‑based care with consistent midwives, the project improved continuity and made antenatal care more accessible for women who struggle with traditional appointment systems.
Quotes: “..a wonderful way to build a community but I also feel like I learned so much more then I would have under any other mode of care. “
“The support from both the midwife’s and other mothers have been invaluable. The pregnancy circle allowed me to have ownership over my pregnancy and make informed choices around my birth. I felt confident in my rights when in labour and felt informed about my choices during birth. “
“I feel the pregnancy circle has better equipped me to cope with becoming a mother and this supported my mental health going into motherhood. I now feel like I have a lovely network of new mums.”
Project: Breastfeeding Padlet
MNVP: Staffordshire & Stoke on Trent MNVP
What? Service user feedback received by the MNVP identified a lack of antenatal breastfeeding information and inconsistent postnatal support across Staffordshire and Stoke-on-Trent. Existing antenatal classes were not equitable, as they were limited to low-risk pathways, leaving a clear information gap. Following the success of a neonatal feeding Padlet, it was proposed that MNVP develop a resource for all families covering breastfeeding. The MNVP, Breastfeeding Network, and Infant Feeding Team at Royal Stoke Maternity Hospital co-produced the Padlet with staff, community teams, and service users over a period of 18 months. The Padlet is accessible to all families via QR code on personal devices or hospital iPads. Staff and community teams use QR code lanyards and posters to promote and signpost the resource. It is available in over 50 languages, with automatic translation based on device settings, alongside additional multilingual resources and provides information from finding support, how to videos, and overcoming breastfeeding challenges. See the padlet here.

Service user involvement: The initial idea for the padlet arose following service user feedback which highlighted a gap in knowledge, support and accessible information. The MNVP held listening sessions within the local community and attended community breastfeeding groups to understand what information families specifically wanted and needed. The padlet was then designed and service users tested its functionality and approved the content.
Staff involved: The Infant Feeding Lead at UHNM worked with the MNVP Lead.
Benefits: The padlet has improved access to consistent, high-quality infant feeding information and support for all families. Early uptake (150+ users since launch) and positive staff feedback indicate it is already enhancing both antenatal discussions and postnatal care. Staff reported strong enthusiasm at launch, highlighting the Padlet as “a valuable resource to offer women support” and “a helpful prompt for antenatal conversations.” It has also been used in clinical settings, including by obstetric staff supporting mothers with mastitis. The Padlet has improved equity, particularly for marginalised groups. Its availability in over 50 languages, with automatic translation, has enabled better support for families whose first language is not English. In addition, as it is accessible via QR code on personal devices and hospital iPads, it helps overcome barriers for those who may not be able to attend antenatal classes or access traditional services.
Project: Neuroinclusive Maternity Passports
Coventry & Warwickshire MNVP
What? In April 2025, the Coventry and Warwickshire MNVP identified, through service user feedback, a gap in support for neurodivergent women and birthing people receiving maternity care. Many ND folk may appreciate subtle adjustments or information about their care but do not want to draw too much attention to the fact. In response, South Warwickshire University NHS Foundation Trust (SWFT), in collaboration with the MNVP and service users, developed the Maternity Passport.
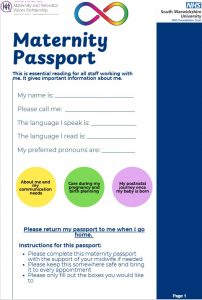
The passport can be completed by anyone who identifies as neurodivergent and serves as an individualised communication tool, providing staff with clear, practical guidance on how best to support their needs. It is paper based and the service user will hold it to share at each stage of their maternity journey.
The Maternity Passport was launched on 13 April 2026, alongside the introduction of Sensory Boxes in each clinical area, providing access to sensory aids for neurodivergent women and birthing people. The IT system has been updated for staff to be able to input when a service user is using a passport so colleagues are aware and can support the service user appropriately. It can be found by scrolling down to the neuro-inclusion support line on the SWFT Public Health padlet here.
Service user involvement: A gap in support for neurodivergent women and birthing people accessing maternity care was initially identified through service user feedback to the Coventry and Warwickshire MNVP.
In response, the Maternity Passport was developed and refined through multiple iterations, informed by feedback from community focus groups led by the MNVP. It was also reviewed by SWFT maternity staff who identify as neurodivergent, including those with recent experience of using maternity services. Engagement Leads (Miryka Yeats – South Warwickshire, Sarah Mair – North Warwickshire, Liz Skidmore – Deputy Strategic Lead and Rugby Engagement Lead) worked with staff to draft a maternity passport and gather examples from elsewhere. A workshop identified elements from these which best met the needs of our local service users.
Staff involved: Claire Morton & Sally Talbot – Public Health Midwives Warwick Hospital The Maternity Passport is being adopted by George Eliot Hospital NHS Trust, a partner Trust within the Foundation Group and LMNS.
Benefits: The Maternity Passport has been introduced to improve the maternity care experience for individuals who identify as neurodivergent. It aims to:
- Reduce anxiety and minimise misunderstandings
- Improve communication between patients and staff
- Support staff in making reasonable adjustments in a timely way
- Promote more person-centred care
Anecdotally the passport has been well received but was only launched in April 2026 so detailed feedback will be collected in due course.
Project: Induction of Labour project
Greater Manchester MNVP
What? We are currently undertaking an project exploring the experience of service users in the induction of labour. The project is following an Experience Based Co-Design (EBCD) approach and has so far included; Engagement with families about their experiences of induction of labour and engagement with maternity staff to understand service perspectives. (See Deduction of Labour video for staff)
Work has identified the emotional touchpoints for both staff and service users within the induction pathway, focusing on the communication barriers and ensuring key information is available in the most accessible way.
We are running a joint staff and service user event on the 5th of May to identify shared priorities for improvement, with those who have already contributed to the project. Following on from this two or three areas of work will be chosen for further focus leading to co produced projects.
Service user involvement: The project came to fruition in direct response to families sharing their experiences of Induction. We held listening events for service users at Manchester Art Gallery , the Whitworth Gallery (pic below), Cheadle Mosque and Children’s Centres, which were advertised on social media networks and well-attended. An online survey was also undertaken.
 A key strand of this activity has been participants consenting to discuss their experiences on camera, so that their views and insights can be initially shared at a joint co production event in May, where further areas of project co production will be identified. We have focused on making these events child-friendly and making it as easy as possible for participants to attend and tell their story.
A key strand of this activity has been participants consenting to discuss their experiences on camera, so that their views and insights can be initially shared at a joint co production event in May, where further areas of project co production will be identified. We have focused on making these events child-friendly and making it as easy as possible for participants to attend and tell their story.
Staff involved: As part of a parallel process, we are working with Edel Dobbin, lead midwife (MU Foundation NHS Trust), who has been instrumental in running a staff survey and hosting multiple workshops with staff from across Greater Manchester involved in the induction pathway. As part of this process we are working closely with the Clinical Lead for Fetal Monitoring and the Clinical Lead Midwife for Greater Manchester.
Benefits: We are carrying out an experience based co design methodology; and, therefore, anticipate that the key learnings will evolve during this research, particularly as we hold our joint staff and service user event to identify priorities for improvement.
We do feel this is an important – and potentially very significant – piece of research. It’s clear from consistent user feedback – as well as anecdotal reports from clinical staff – that this is a topic where miscommunication can be common and have negative outcomes. This co-produced research will identify the pinch points, allow clearer communication around consent and what to expect in terms of the process – as well as giving clinical staff a better understanding of likely barriers.
Project: Improvement to Discharge Process
Lister MNVP
What? Lister MNVP worked with East and North Hertfordshire Teaching NHS Trust maternity teams to improve communication on the postnatal ward following feedback from women and families. Women reported poor communication and uncertainty around discharge, particularly not knowing what was still outstanding for themselves or their baby, or why delays were occurring. In response, Lister MNVP co-produced: * A “Going Home” discharge video accessible by QR code * A “Journey Home After Birth” discharge checklist outlining all discharge steps for mum and baby. These resources improved communication, helped families better understand the discharge process and delays, and supported a more positive postnatal experience. This work formed part of a wider postnatal discharge pathway improvement initiative focused on reducing delays caused by system and process issues rather than clinical need. A Rapid Process Improvement Workshop involving staff and service users reviewed discharge pathways, identified causes of delays and developed practical improvements to communication and coordination. (See Lister MNVP Facebook page and video here)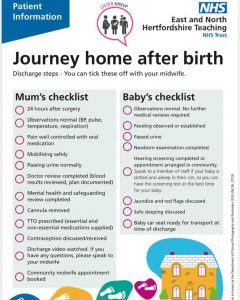
Service user involvement: Service users were involved throughout the project through feedback gathered by Lister MNVP via walk the patch engagement, surveys and wider community engagement activities with women and families using maternity services. Feedback identified concerns around poor communication on the postnatal ward, uncertainty about discharge processes and lack of understanding around delays. Women and families shared their experiences directly with the MNVP, highlighting the need for clearer and more consistent discharge information. This feedback informed discussions and collaborative working with maternity staff to co-produce the discharge video and “Journey Home After Birth” checklist, ensuring the resources reflected the needs and experiences of service users.
Staff involved: East and North Hertfordshire Teaching NHS Trust: Midwives, Maternity Support Workers (MSWs), Nursery staff, Obstetricians, Pharmacists, Communications team, Postnatal Ward Manager. These teams worked collaboratively with service users and MNVP representatives to review discharge pathways, identify communication challenges and co-produce improvements to the postnatal discharge experience.
Benefits: The co-produced discharge video and “Journey Home After Birth” checklist improved communication and transparency for women and families on the postnatal ward. Families had clearer information about what was still outstanding for discharge for both mum and baby, helping reduce uncertainty, anxiety and frustration around delays. The resources also helped provide more consistent information from staff and supported women to feel more informed and prepared when going home after birth.
Feedback from service users included:
“It helped to know what we were still waiting for before discharge.”
“The checklist made things much clearer and reduced stress.”
“Having information to look back at was really helpful when overwhelmed after birth.”
The use of accessible, visual and easy-to-follow resources also supported improved understanding for families who may find verbal information difficult to retain during the immediate postnatal period, helping make communication more inclusive and equitable.